The Viral Connection:
When Co-Infections Become Catalysts for Cancer
Cancer is one of the leading causes of death worldwide, and its origins are as diverse as the disease itself, ranging from inherited mutations to viral infection. Fundamentally, cancer arises when the body’s regulatory systems fail to keep cell growth and repair in balance, leading to uncontrolled proliferation. This breakdown can be driven by genetic mutations (inherited or acquired), environmental exposures such as radiation or carcinogenic chemicals, and lifestyle factors like smoking, alcohol use, diet, and obesity. Meridian Life Science, a leader in ambient-temperature–stable reagent technologies, supports this mission with solutions that advance both immunoassay and molecular diagnostics. Infectious causes of cancer, particularly viruses known as oncoviruses, are less widely recognized but increasingly important. Globally, about 1 in 6 cancers (12–20%) are linked to viral infections1, making infection the third leading cause of cancer worldwide. While lifestyle-related and environmental/genetic factors typically drive cancer through mutations, they can also induce epigenetic changes—such as silencing of tumor suppressor genes—that contribute to cancer development.
The Role of Oncoviruses
Epstein–Barr virus (EBV) was the first virus confirmed to cause human cancer, and it remains one of the best-studied examples of viral oncogenesis. Today, the International Agency for Research on Cancer (IARC) identifies seven viruses as Group 1 carcinogens: HPV, HBV, HCV, EBV, Kaposi sarcoma–associated herpesvirus (KSHV/HHV-8), HTLV-1, and HIV. Collectively, these viruses are linked to cancers including hepatocellular carcinoma, gastric cancer, cervical cancer, nasopharyngeal carcinoma, Kaposi sarcoma, lymphoma, and adult T-cell leukemia/lymphoma2. Most people will contract at least one oncogenic virus during their lifetime, and in most cases these infections resolve within months without progressing to cancer. However, some oncoviruses establish lifelong infections and, under certain conditions such as immune suppression, chronic inflammation, or exposure to co-oncogenic factors, infected cells can acquire malignant traits that drive cancer development. Malignant transformation can occur through direct pathways, including viral gene integration into the host genome, disruption of tumor suppressor genes, activation of oncogenes, and interference with cell-cycle regulation. Indirect mechanisms include the establishment of persistent infections that promote chronic inflammation, immune suppression, and genomic instability, all of which create a permissive environment for oncogenesis. Despite significant advances, the molecular mechanisms underlying viral oncogenesis remain only partially understood, underscoring the complexity of virus–host interactions.An overview of viral oncogenic mechanisms.
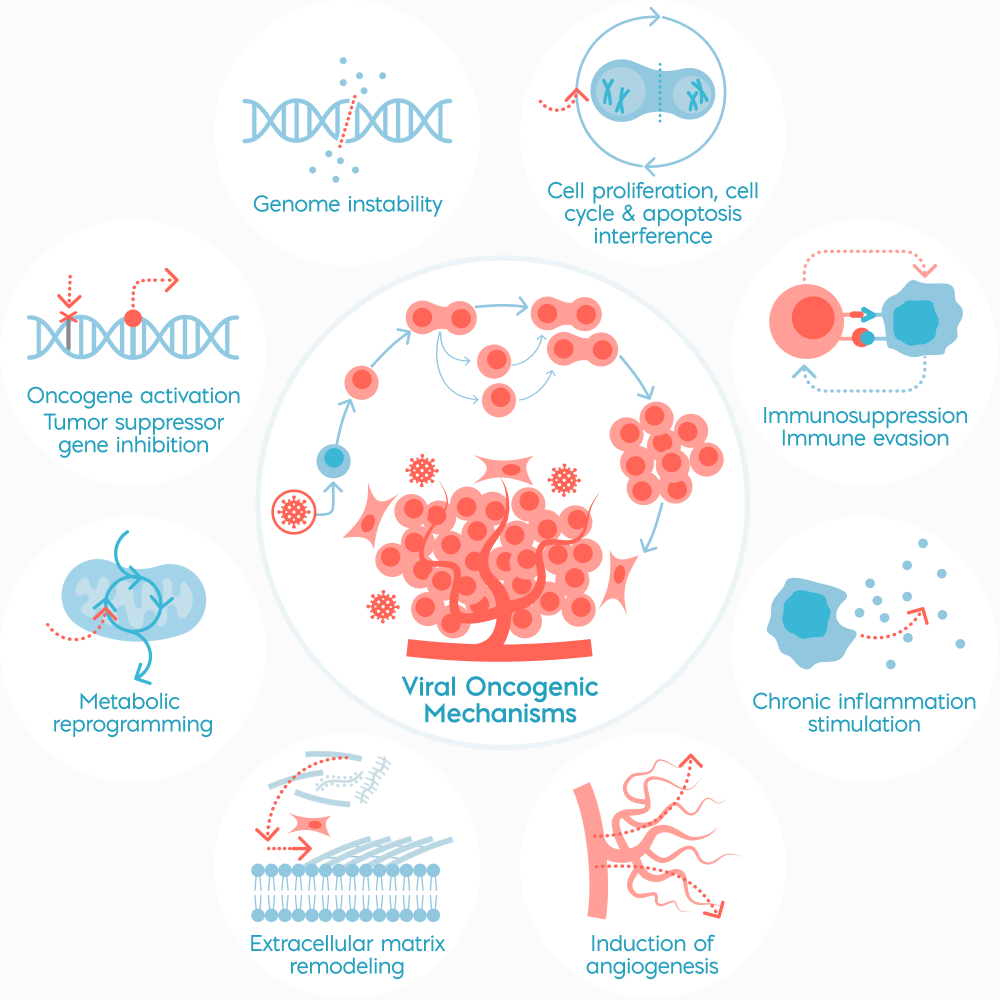
Oncoviruses transform host cells by disrupting normal controls—activating oncogenes, silencing tumor suppressors, driving chronic inflammation, and evading immune responses. Together, these mechanisms promote tumor development and metastasis: direct oncogenesis and indirect oncogenesis. This figure was adapted from: https://www.nature.com/articles/s41392-025-02197-9/figures/3
The Global Burden of Oncoviruses and Co-Infections
Oncoviruses are responsible for approximately 2 million new cancer cases annually3, with the heaviest burden in low- and middle-income countries where vaccination and screening remain limited. Of the seven viruses as Group 1 carcinogens:
- HPV accounts for ~5% of cancers worldwide, driving cervical cancer and contributing to anal, oropharyngeal, penile, vulvar, and vaginal cancers
- HBV and HCV together cause up to 80% of hepatocellular carcinoma, one of the deadliest cancers, often diagnosed at late stages
- EBV, carried by over 90% of people globally, is linked to lymphomas and nasopharyngeal carcinoma
- HHV-8 causes Kaposi’s sarcoma, particularly in HIV-positive individuals
- HTLV-1 is less common but can trigger aggressive adult T-cell leukemia/lymphoma
- Merkel cell polyomavirus (MCPyV) is the main cause of Merkel cell carcinoma, a rare but highly lethal skin cancer
- HIV although not oncogenic, causes immune suppression that magnifies the risk of cancers caused by these viruses
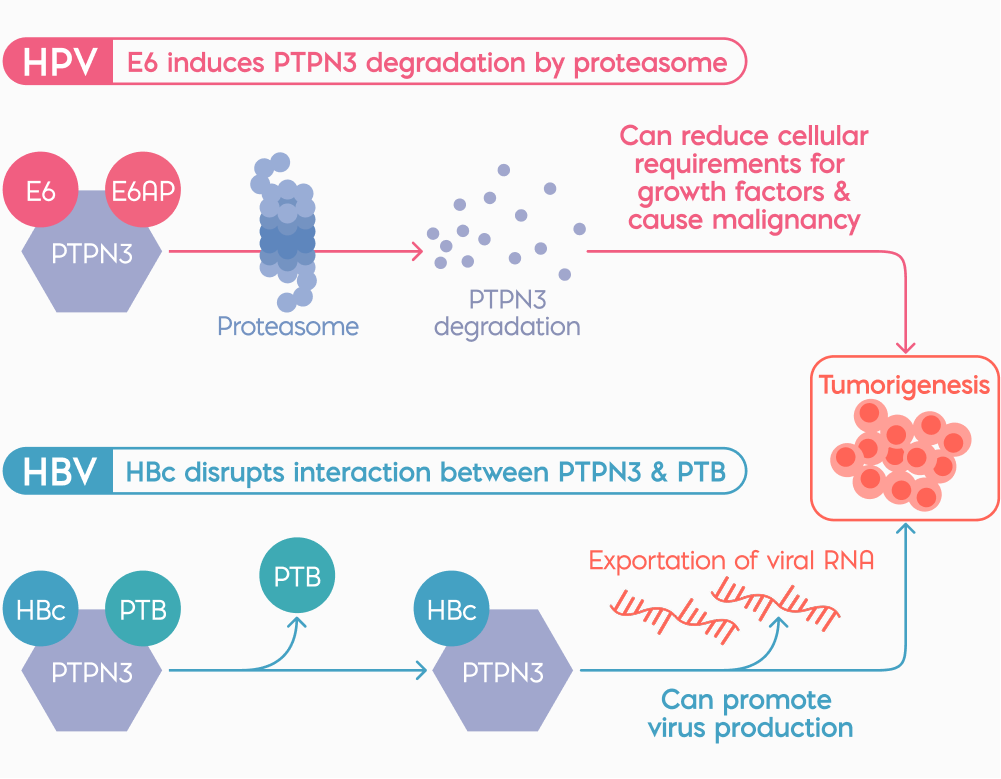
Figure 1. Schematic of potential commonalities in the molecular mechanisms between HPV and HBV in tumorigenesis. https://pmc.ncbi.nlm.nih.gov/articles/PMC10783544/
Co-Infections and Viral Synergy
Co-infections create unique biological conditions in which viruses can act synergistically, even without infecting the same cell. Virus-infected cells release cytokines, chemokines, exosomes, and other signaling molecules that reshape the tumor microenvironment and influence neighboring cells.
One example is the interaction between HIV and HHV-8: HIV-induced immune suppression provides the ideal environment for HHV-8 to drive Kaposi’s sarcoma. Similarly, patients infected with both HBV and HCV face a much greater risk of liver cancer than those with either virus alone, as HBV integrates into host DNA while HCV promotes chronic inflammation creating two complementary pathways to tumor formation. HIV can also worsen HPV-driven cancers, including cervical and anal cancer, by reducing the body’s ability to clear precancerous lesions.
Adding to this complexity, research suggests that some co-infections may influence cancer development even without the continued presence of the second pathogen—a phenomenon described as the “hit-and-run” theory (https://pmc.ncbi.nlm.nih.gov/articles/PMC10783544/). This highlights the potential for viral synergy, where, in this case, individuals with HPV who also carry other oncoviruses face not only an increased risk of HPV-associated cancers but also additional malignancies.
Complicating matters further, emerging evidence indicates that SARS-CoV-2, though not itself an oncovirus, can reactivate latent oncoviruses such as EBV and HHV-84. The immune dysregulation triggered by SARS-CoV-2 appears capable of awakening dormant viruses, indirectly elevating cancer risk in vulnerable populations. These findings illustrate how interactions between oncogenic and non-oncogenic viruses can further shape cancer development and outcomes, underscoring the complexity of virus-driven oncogenesis.
Prevention and Diagnosis of Virus-Driven Cancers
Preventing and diagnosing oncovirus-driven cancers requires a different approach than treating traditional cancers. For patients with viral co-infections, the prognosis is often worse than with single infections. These cancers develop faster, are diagnosed later, and respond less well to treatment. Vaccination programs against HPV and HBV have already shown dramatic reductions in infection rates and related cancers, but broader coverage, especially in low-resource regions, is essential. For viruses without vaccines, such as HCV or EBV, early screening and antiviral therapies play a critical role in lowering long-term cancer risk. On the diagnostic side, relying on single-pathogen testing is often inadequate when multiple infections may be present. Instead, syndromic and multiplex panels that can detect several viruses at once, give clinicians a clearer picture of a patient’s risk and enable earlier intervention. Combined with better surveillance and education, these tools make it possible to not only prevent many viral cancers but also catch them before they progress to late, hard-to-treat stages.
Commercial immunoassay technologies that enable multiplex detection are already available, though most are still geared toward research rather than clinical diagnostics. Platforms such as Bio-Rad’s Bio-Plex, Meso Scale Discovery (MSD) kits, and Merck’s Milliplex assays allow simultaneous measurement of multiple viral or cancer-related biomarkers from a single sample, while Randox’s STI Array demonstrates how syndromic panels can be applied clinically by detecting up to ten sexually transmitted pathogens at once. However, fully validated immunoassays that specifically combine oncoviruses and co-infection panels for cancer risk assessment remain limited, with most solutions currently used in research, surveillance, or specialized testing settings. This highlights both the technical feasibility of multiplex immunoassays and the urgent need to expand them into routine cancer diagnostics.
For immunoassays, the future is moving toward portable, multiplex-capable formats that bring testing closer to patients. One example is the development of “lab-in-a-box” platforms which are compact, self-contained systems that automate sample preparation, detection, and readout making syndromic viral panels feasible even in low-resource settings. Sensitivity is also being advanced through new labeling technologies, including fluorescent nanoparticles, quantum dots, and magnetic particles, which help reduce background noise. At the same time, smartphone-based readers and portable optical devices are being paired with strips to minimize user interpretation errors and deliver semi-quantitative results5.
Further gains are being made in assay reliability, with improvements in membrane chemistry and blocking agents enhancing reproducibility6 and accuracy while the integration of isothermal amplification and CRISPR-based methods7 is dramatically boosting sensitivity. Taken together, these innovations are transforming lateral flow from a simple yes/no test into a powerful multiplexed platform for near-patient diagnostics, capable of tackling complex challenges like viral co-infections.
Co-Infections and Viral Synergy
Co-infections create unique biological conditions in which viruses can act synergistically, even without infecting the same cell. Virus-infected cells release cytokines, chemokines, exosomes, and other signaling molecules that reshape the tumor microenvironment and influence neighboring cells. One example is the interaction between HIV and HHV-8: HIV-induced immune suppression provides the ideal environment for HHV-8 to drive Kaposi’s sarcoma. Similarly, patients infected with both HBV and HCV face a much greater risk of liver cancer than those with either virus alone, as HBV integrates into host DNA while HCV promotes chronic inflammation creating two complementary pathways to tumor formation. HIV can also worsen HPV-driven cancers, including cervical and anal cancer, by reducing the body’s ability to clear precancerous lesions. Adding to this complexity, research suggests that some co-infections may influence cancer development even without the continued presence of the second pathogen—a phenomenon described as the “hit-and-run” theory (https://pmc.ncbi.nlm.nih.gov/articles/PMC10783544/). This highlights the potential for viral synergy, where, in this case, individuals with HPV who also carry other oncoviruses face not only an increased risk of HPV-associated cancers but also additional malignancies. Complicating matters further, emerging evidence indicates that SARS-CoV-2, though not itself an oncovirus, can reactivate latent oncoviruses such as EBV and HHV-84. The immune dysregulation triggered by SARS-CoV-2 appears capable of awakening dormant viruses, indirectly elevating cancer risk in vulnerable populations. These findings illustrate how interactions between oncogenic and non-oncogenic viruses can further shape cancer development and outcomes, underscoring the complexity of virus-driven oncogenesis.Prevention and Diagnosis of Virus-Driven Cancers
Preventing and diagnosing oncovirus-driven cancers requires a different approach than treating traditional cancers. For patients with viral co-infections, the prognosis is often worse than with single infections. These cancers develop faster, are diagnosed later, and respond less well to treatment. Vaccination programs against HPV and HBV have already shown dramatic reductions in infection rates and related cancers, but broader coverage, especially in low-resource regions, is essential. For viruses without vaccines, such as HCV or EBV, early screening and antiviral therapies play a critical role in lowering long-term cancer risk. On the diagnostic side, relying on single-pathogen testing is often inadequate when multiple infections may be present. Instead, syndromic and multiplex panels that can detect several viruses at once, give clinicians a clearer picture of a patient’s risk and enable earlier intervention. Combined with better surveillance and education, these tools make it possible to not only prevent many viral cancers but also catch them before they progress to late, hard-to-treat stages. Commercial immunoassay technologies that enable multiplex detection are already available, though most are still geared toward research rather than clinical diagnostics. Platforms such as Bio-Rad’s Bio-Plex, Meso Scale Discovery (MSD) kits, and Merck’s Milliplex assays allow simultaneous measurement of multiple viral or cancer-related biomarkers from a single sample, while Randox’s STI Array demonstrates how syndromic panels can be applied clinically by detecting up to ten sexually transmitted pathogens at once. However, fully validated immunoassays that specifically combine oncoviruses and co-infection panels for cancer risk assessment remain limited, with most solutions currently used in research, surveillance, or specialized testing settings. This highlights both the technical feasibility of multiplex immunoassays and the urgent need to expand them into routine cancer diagnostics. For immunoassays, the future is moving toward portable, multiplex-capable formats that bring testing closer to patients. One example is the development of “lab-in-a-box” platforms which are compact, self-contained systems that automate sample preparation, detection, and readout making syndromic viral panels feasible even in low-resource settings. Sensitivity is also being advanced through new labeling technologies, including fluorescent nanoparticles, quantum dots, and magnetic particles, which help reduce background noise. At the same time, smartphone-based readers and portable optical devices are being paired with strips to minimize user interpretation errors and deliver semi-quantitative results5. Further gains are being made in assay reliability, with improvements in membrane chemistry and blocking agents enhancing reproducibility6 and accuracy while the integration of isothermal amplification and CRISPR-based methods7 is dramatically boosting sensitivity. Taken together, these innovations are transforming lateral flow from a simple yes/no test into a powerful multiplexed platform for near-patient diagnostics, capable of tackling complex challenges like viral co-infections.Conclusion
Viral co-infections represent a hidden multiplier of cancer risk, underscoring the need for innovative tools that extend beyond conventional diagnostics. At Meridian, we support both immunoassay and molecular diagnostics across a broad range of cancer biomarkers and oncovirus targets (EBV, HBV, HCV, HPV, HTLV-1, and HIV), providing assay developers with the reagents needed to improvehttps://www.meridianbioscience.com/lifescience/products/antibodies-antigens/viral-hepatitis/hepatitis-c/ sensitivity, specificity, and reliability.
Our portfolio spans a comprehensive range of antigens, antibodies, enzymes, and master mixes, complemented by interference blockers that enhance assay precision and reproducibility. These reagents support a wide spectrum of diagnostic applications, including point-of-care multiplex lateral flow and LAMP assays to high-throughput immunoassays and molecular qPCR, facilitating the creation of robust, scalable assays for cancer biomarker detection.
As a leader in ambient-temperature–stable molecular technologies, including first-to-market master mixes and enzymes, Meridian enables assay developers to design reliable, high-performance assays that eliminate cold-chain requirements, improving accessibility and cost efficiency. By advancing diagnostic innovation, Meridian supports global efforts to improve early detection, expand access, and strengthen surveillance of virus-driven cancers.
References:
1. Dai, L., Wilson, L. G., Nakagawa, M., & Qin, Z. (2024). Coinfections with additional oncoviruses in HPV+ individuals: Status, function, and potential clinical implications. Journal of Medical Virology, 96(1), e29363. https://doi.org/10.1002/jmv.29363
2. Xiao, Q., Liu, Y., Li, T., & et al. (2025). Viral oncogenesis in cancer: From mechanisms to therapeutics. Signal Transduction and Targeted Therapy, 10, 151. https://doi.org/10.1038/s41392-025-02197-9
3. Contreras, A., Amaya Sánchez, S., Rodríguez-Medina, C., & Botero, J. E. (2024). The role and impact of viruses on cancer development. Periodontology 2000. Advance online publication. https://doi.org/10.1111/prd.12566https://pmc.ncbi.nlm.nih.gov/articles/PMC10178366/
4. Park, J. (2022). Lateral flow immunoassay reader technologies for quantitative point-of-care testing. Sensors, 22(19), 7398. https://doi.org/10.3390/s22197398
5. Khatmi, G., Klinavičius, T., Simanavičius, M., et al. (2024). Lateral flow assay sensitivity and signal enhancement via laser µ-machined constrains in nitrocellulose membrane. Scientific Reports, 14, 22936. https://doi.org/10.1038/s41598-024-61891-0
6. Yigci, D., Atçeken, N., Yetisen, A. K., et al. (2023). Loop-mediated isothermal amplification-integrated CRISPR methods for infectious disease diagnosis at point of care. ACS Omega, 8(46), 43357–43373. https://doi.org/10.1021/acsomega.3c04422